Hospitals Are Adding Billions in ‘Facility’ Fees for Routine Care
Apr 11, 2024
Unsuspecting
patients find themselves at the mercy of institutions tacking on the bills
Tim Ebel’s visit with an ear, nose and throat specialist at an Ohio
clinic last October came to $348. At the same time, he got a second bill for
$645.
The
hospital system that owns the Avon, Ohio, clinic had charged him separately for
use of the office where he met his physician. It is what is known as a facility
fee, which included overhead for the system’s hospitals though Ebel hadn’t set
foot in one.
His wife, Kelly Ebel, tried to
get the system, University Hospitals, to waive or mark down the fee. It
refused.
“When they do something like this,
to her and I, it’s not fair,” Tim Ebel said. “This is not how you bring down
medical costs in this country.”
Hospitals are adding billions of
dollars in facility fees to medical bills for routine care in outpatient
centers they own. Once an annoyance, the fees are now pervasive, and in some
places they are becoming nearly impossible to avoid, data compiled for The Wall
Street Journal show. The fees are spreading as hospitals press on with
acquisitions, snapping up medical groups and tacking on the additional
charges.
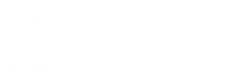
The fees raise prices by hundreds
of dollars for widely used and standard medical care, including colonoscopies,
mammograms and heart screening.
The added cost isn’t justified, physicians and economists say.
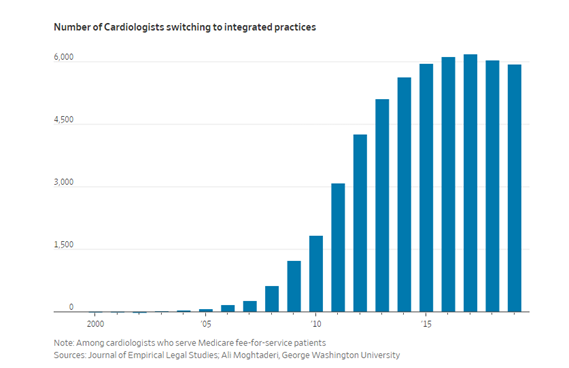
Medicare advisers said last year the federal insurer likely overpaid for a
sample of services by about $6 billion because of the fees in 2021.
“You’re
not getting anything extra,” said Loren Adler, a health economist at the
Brookings Institution, who studies hospital billing.
Hospitals
say facility fees help offset the extra costs that they incur to meet federal
regulations. “It’s not as simple as same services, across-the-board,”
said Jason Kleinman, director of federal relations for the American
Hospital Association.
Fees on outpatient services also help to cover costly hospital
services like neonatal intensive-care units, he said.
A
spokeswoman for University Hospitals, based in Cleveland, said it is aware the
facility fees can increase patients’ out-of-pocket expenses and the system
seeks to lower healthcare spending. “We are always conscious of the rising cost
of healthcare in the United States,” she said.
Kelly
Ebel isn’t having it. “Quit gouging us,” she said.
The
fees show up on patients’ bills after hospitals snap up clinics and doctors.
Hospitals can designate the newly acquired clinics as an extension of their
operations, forcing patients to pay the fees to cover costs for the entire
hospital.
Fees
have grown more pervasive as hospitals have gone on an acquisition tear in
recent years, chasing
after patients who have more options to get medical care somewhere
else. Many hospital systems now get at least half their revenue from patients
who aren’t admitted. By one estimate, more than half of doctors work for
hospitals.
That
gives hospitals more opportunities to apply fees—and generate revenue. For
chemotherapy given by infusion, more than half of bills now have facility fees,
among patients who are covered by traditional Medicare or some of the
largest U.S.
health insurers. About a decade ago, it was roughly one-third to 45%,
according to Medicare’s advisory commission and the Health Care Cost Institute,
a nonprofit that analyzes data from health insurers.
In
some states, fees have spread even further. In Ohio and Maine, facility fees
are tacked onto roughly four of every five bills sent to each state’s largest
insurer for heart-disease screening, according to data compiled for the Journal
by Elevance Health, the
parent company of a major health insurer.
Not
all hospital-owned clinics apply the fees. Avoiding them is an exercise in
frustration, patients say. Many discover them only when getting the bill.
“I
figured it was a mistake,” said Matthew Burin, who got billed $750 by an
orthopedic clinic after his son, then 8, broke an arm. The total included a
$400 facility fee for Children’s Hospital Colorado. He disputed it and won, he
said.
Six years later, he remains on
guard for the fees. “Every appointment I make, the first question I ask is do
you charge facility fees?”
Indiana
banned the fees at clinics located off hospital campuses for the
largest nonprofit health systems, starting next year. Some states prohibit fees
for telehealth or preventive care. Others require hospitals to notify patients
of fees before treatment.
Under
a new state law in Colorado, hospitals in the state will have to disclose the
facility fees starting in July.
Children’s
Hospital Colorado said it would add new disclosures into its cost estimates for
patients. It said it bills patients for hospital overhead because its
clinics provide specialized services, and because it doesn’t employ its
doctors, who bill separately.
Lawmakers
and Congress have proposed limiting fees covered by Medicare, which advisers to
the federal insurer have unanimously recommended. Under a bill passed by the
House in December, Medicare would no longer pay hospital facility fees for
chemotherapy and other drugs infused by doctors in clinics off a hospital
campus, saving about $3.7 billion over 10 years.
The American Hospital Association opposes limiting the fees, saying
restrictions would cut revenue to hospitals already squeezed financially by high
labor costs and inflation.
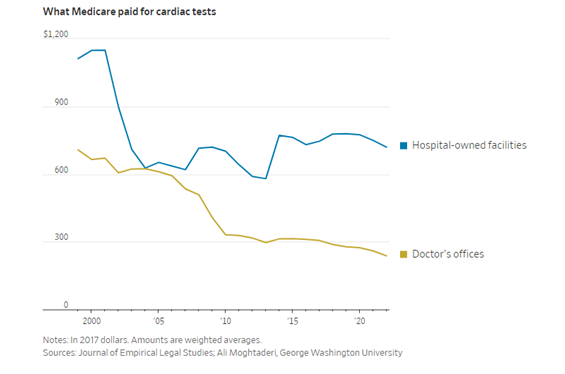
The
prospect of extra revenue from the fees has helped drive hospitals to snap up
groups of heart doctors, according
to a study published last year in the Journal of Empirical Legal
Studies.
A
shift in physician employment by hospitals is now rapidly playing out for cancer
doctors in North Carolina, a preliminary analysis for the Journal by
one of the study’s researchers found.
Roughly 80% of oncologists in the Charlotte, N.C., area work for
hospitals, up from half about 10 years earlier.
Among
the North Carolina hospital systems that have been buying up oncologists is
Novant Health, which employed 75 cancer specialists at the end of the last
decade, up from seven in 2010. One of the cancer clinics Novant bought: Lake
Norman Oncology in suburban Charlotte, N.C.
After
the acquisition, in December 2020, Lake Norman billed Rebecca Smith, a
breast cancer survivor, roughly $400 for monitoring, up from the $76 her
previous visits had cost.
Smith
refused to pay. She said Novant reminded her she had agreed in writing to cover
the bills and sent debt collectors after the single mother.
Smith, a self-employed tax accountant, already paid $1,200 a month
to buy health insurance for herself and her daughter. The new fees were too
much additional expense. “I do not want to leave, but Novant has made it clear
to me that there is no alternative since they turned your practice into a
hospital facility,” she wrote her doctor.
A
Novant Health spokeswoman said it invests in clinics it acquires, and only
levies fees across 10% of about 700 locations. It said patients should work
with their insurers to understand what they will owe out-of-pocket.
Smith moved to Southern Oncology Associates, a medical group owned
by William Mitchell, one of its four physicians. She asked almost
immediately about hospital fees before she scheduled a new appointment.
Mitchell
said he is working to keep the group independent by adding new locations where
clinics don’t compete directly with hospitals. “You sell because you have no
choices,” he said. “I don’t want that.”
Source: Wall Street Journal
Tags: